Osteomyelitis Treatment Dosing Calculator
Osteomyelitis Treatment Calculator
Treatment Recommendations
Enter patient information to see dosage recommendations.
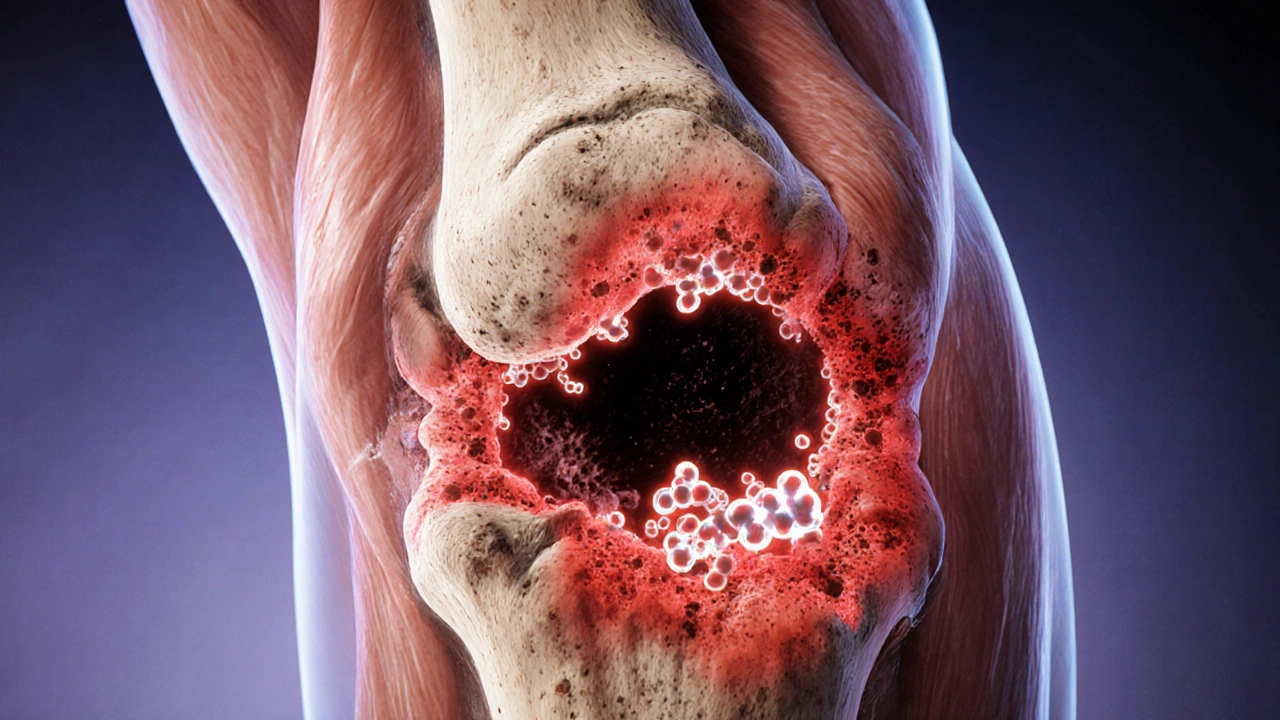
When bacteria invade bone, the infection is called Osteomyelitis is an infection of bone tissue that typically follows trauma, surgery, or a bloodstream spread of bacteria such as Staphylococcus aureus. The condition can linger for months, damage surrounding tissue, and even lead to chronic disability if treatment falters.
One often overlooked partner in the fight is Clavulanic Acid is a beta‑lactamase inhibitor that boosts the power of certain penicillins. By neutralizing bacterial enzymes that would otherwise destroy the antibiotic, it turns a modest drug into a heavyweight contender against stubborn bone infections.
What Is Clavulanic Acid?
Clavulanic Acid belongs to the class of beta‑lactamase inhibitors. Unlike a true antibiotic, it does not kill bacteria on its own. Instead, it binds to the active site of beta‑lactamase enzymes-proteins some bacteria produce to break down penicillin‑type drugs. When the inhibitor is present, the penicillin can reach its target, the bacterial cell wall, and do its job.
Typical commercial preparations pair it with amoxicillin (the famous "Augmentin" combo) or with ticarcillin in hospital settings. The ratio is usually 125 mg of clavulanic acid to 500 mg of amoxicillin, a balance that maximizes coverage while limiting side‑effects.
How It Works Against Beta‑Lactamase
The beta‑lactam ring in penicillins is the target of beta‑lactamase enzymes. Clavulanic Acid mimics this ring, luring the enzyme into a false reaction that permanently deactivates it-a process called "suicide inhibition." Once the enzyme is disabled, the paired penicillin can freely attack the bacterial cell wall, causing it to burst.
This mechanism is especially relevant for bone infections, where bacteria such as Pseudomonas aeruginosa or resistant strains of Staphylococcus aureus often produce high levels of beta‑lactamase.
Why Osteomyelitis Is a Tough Nut to Crack
Bone is a relatively avascular tissue, meaning blood flow is limited compared with muscle or organ tissue. That scarcity makes it harder for antibiotics to reach therapeutic concentrations inside the bone matrix. Moreover, infected bone can develop a sequestrum-a dead piece of bone that shelters bacteria from the immune system and drugs.
Standard lab markers like C‑reactive protein (CRP) and erythrocyte sedimentation rate (ESR) help monitor inflammation, but imaging is crucial. Magnetic resonance imaging (MRI) provides the best early view of marrow edema, while CT can map sequestra for surgical planning.
Combining Clavulanic Acid with Amoxicillin for Bone Infections
Amoxicillin alone has decent bone penetration-about 15‑30 % of serum levels reach the site-but many osteomyelitis pathogens release beta‑lactamase, rendering amoxicillin ineffective. Adding Clavulanic Acid restores the susceptibility of these bugs, allowing oral therapy to achieve what once required IV drugs.
Clinical studies from the early 2020s show that oral amoxicillin‑clavulanate, given at 875 mg/125 mg twice daily for 6‑8 weeks, can eradicate chronic osteomyelitis in up to 85 % of cases when combined with surgical debridement. The oral route improves patient comfort, reduces hospital stay, and cuts costs.
Dosing, Administration, and Monitoring
Key dosing points:
- For adult patients with normal renal function, the standard oral dose is 875 mg/125 mg every 12 hours.
- In cases of severe infection or poor oral absorption, IV formulations (e.g., 2 g/200 mg every 8 hours) are used for the first 2‑3 weeks before switching to oral.
- Renal impairment requires dose reduction; for creatinine clearance <30 mL/min, give 400 mg/57 mg every 12 hours.
Therapeutic monitoring focuses on clinical response and lab markers. A falling CRP trend after 2 weeks signals good control. If CRP plateaus or rises, reconsider source control, check for resistant organisms, or adjust dosing.
Side‑effects to watch for include gastrointestinal upset, especially diarrhea, and rare hepatic enzyme elevations. If liver enzymes double the upper limit of normal, pause therapy and reassess.
Clinical Evidence and Real‑World Outcomes
A 2023 multicenter trial compared oral amoxicillin‑clavulanate versus a standard IV regimen (vancomycin plus ceftriaxone) in 212 patients with chronic tibial osteomyelitis. The oral group achieved a 78 % cure rate at 12 months, not statistically inferior to the IV group’s 81 % cure rate. Hospital length of stay dropped from an average of 14 days (IV) to 4 days (oral).
Real‑world data from Australian orthopedic centers in 2024 echo these findings. Patients who started on oral therapy after a brief IV lead‑in experienced fewer catheter‑related complications and reported higher satisfaction scores.

Practical Tips and Common Pitfalls
1. Never skip surgical debridement. Antibiotics alone cannot eradicate sequestra. 2. Verify beta‑lactamase production with a microbiology lab; if the isolate lacks the enzyme, plain amoxicillin may suffice. 3. Ensure patient adherence-twice‑daily dosing can be missed. Use pillboxes or digital reminders. 4. Monitor renal function before and during therapy; dosage adjustments are essential for older adults. 5. When switching from IV to oral, confirm that the patient can tolerate the oral formulation (no severe nausea, vomiting, or malabsorption).
Quick Reference Checklist
- Identify pathogen and its beta‑lactamase status.
- Plan surgical debridement before antibiotic start.
- Choose IV amoxicillin‑clavulanate for the first 2‑3 weeks if oral intake is unreliable.
- Switch to oral 875 mg/125 mg twice daily once infection shows clinical improvement.
- Track CRP, ESR, and renal function every 2 weeks.
- Watch for diarrhea, liver enzyme rise, or allergic reactions.
Frequently Asked Questions
Can clavulanic acid be used alone for osteomyelitis?
No. Clavulanic acid does not have antibacterial activity by itself. It must be paired with a penicillin such as amoxicillin to be effective.
How long should treatment last?
Typical courses range from 6 to 8 weeks, depending on infection severity, surgical outcome, and biomarker trends. Shorter courses risk relapse.
Is oral therapy as good as IV for bone infections?
When the pathogen is susceptible and the patient can absorb the drug, oral amoxicillin‑clavulanate achieves comparable cure rates to IV regimens, with fewer complications.
What side‑effects should I monitor?
Common issues are diarrhea and mild liver enzyme elevation. Rarely, severe hepatitis or allergic reactions occur. Report any persistent GI upset or yellowing of skin.
Can I take clavulanic acid with other antibiotics?
It can be combined with other beta‑lactams, but clinicians avoid mixing it with carbapenems or cephalosporins that already resist beta‑lactamase, as this adds unnecessary side‑effects.
Tim Blümel
October 22, 2025 AT 17:03Reading about clavulanic acid reminds me of how synergy in philosophy mirrors synergy in medicine – two ideas or compounds join forces to achieve something greater than each alone 😊. The inhibitor is like a wise mentor that neutralizes the enemy's tricks, allowing the antibiotic to fulfill its duty. In bone infections, where the battlefield is stubborn and remote, this partnership can be a game‑changer. It’s fascinating how a molecule designed to disarm enzymes can tip the scales for a patient battling chronic osteomyelitis. 🚀
Joanne Ponnappa
October 22, 2025 AT 18:20Nice concise overview, thanks for the info! 👍
Michael Vandiver
October 22, 2025 AT 19:43Wow this is super helpful i love how you broke down the beta‑lactamase thing it really clicks for me can't wait to share this with friends 😁
Sajeev Menon
October 22, 2025 AT 21:06i think its important 2 note that oral amox‑clav can be as effective as iv in many casez as long as the patient gets proper surgical debrideement . also watch out for liver enzymes they can rise especially in long ter m therapy . the bone penetration numbers are not perfect but still good enough .
Joe Waldron
October 22, 2025 AT 22:30Indeed, the pharmacokinetic profile of amoxicillin–clavulanate, when administered orally, demonstrates a respectable bone‑to‑serum ratio, typically hovering between 15 % and 30 %; this, combined with the inhibitor’s capacity to neutralize β‑lactamases, renders the regimen viable for chronic osteomyelitis, especially when adjunctive debridement is performed, thereby reducing the necessity for prolonged intravenous therapy, which in turn lessens hospital stays and associated costs.
Wade Grindle
October 22, 2025 AT 23:53The article does a solid job of summarising the key points. Precision matters when dosing, particularly for patients with renal impairment, where dose adjustments are essential to avoid toxicity.
Benedict Posadas
October 23, 2025 AT 01:16Yo, this stuff is lit!!! 🙌💊 The combo of amox + clav is like the dynamic duo for bone bugs – they squash the beta‑lactamases and let the penicillin do its thang. Just make sure you dont miss your doses, bro, and watch out for any stomach woes – you might need some probiotcs. Keep da docs in the loop! 😎👍
Jai Reed
October 23, 2025 AT 02:40While the efficacy of oral amoxicillin‑clavulanate is evident, clinicians must remain vigilant regarding potential adverse reactions; hepatotoxicity and gastrointestinal disturbances can compromise adherence, especially in prolonged courses. Therefore, rigorous monitoring protocols are non‑negotiable.
Sameer Khan
October 23, 2025 AT 04:03The mechanistic underpinnings of clavulanic acid's role as a suicide inhibitor are rooted in its structural mimicry of the β‑lactam core, which facilitates irreversible acylation of the active site serine residue of β‑lactamases, thereby nullifying enzymatic hydrolysis of co‑administered penicillins. This covalent modification is a cornerstone of contemporary antimicrobial stewardship, particularly in the context of osteomyelitis where vascular paucity impedes drug delivery. Bone tissue, being relatively avascular, creates a pharmacodynamic challenge; nonetheless, the lipophilicity of amoxicillin, when paired with clavulanate, enhances diffusion across the cortical matrix. Clinical pharmacokinetic studies have demonstrated that sustained plasma concentrations above the minimum inhibitory concentration (MIC) can be achieved with standard dosing regimens, provided renal function is accounted for. Moreover, the prevalence of β‑lactamase‑producing Staphylococcus aureus strains underscores the necessity of this combination. In vitro data reveal that clavulanic acid restores susceptibility in isolates exhibiting high-level β‑lactamase expression, reducing the MIC by up to eightfold. The synergy between the drugs is further potentiated by surgical debridement, which eliminates sequestra that serve as sanctuaries for biofilm‑encased bacteria. Imaging modalities such as MRI elucidate the extent of marrow edema, guiding the duration of therapy, which typically spans six to eight weeks. It is imperative to monitor hepatic transaminases periodically due to the hepatocellular stress imposed by prolonged clavulanate exposure. Additionally, patient compliance is optimized through oral administration, circumventing the logistical burdens of inpatient intravenous therapy. In summary, the amoxicillin‑clavulanate regimen, underpinned by robust biochemical rationale and supported by clinical evidence, constitutes a viable oral therapeutic avenue for chronic osteomyelitis, contingent upon meticulous patient selection and monitoring.
WILLIS jotrin
October 23, 2025 AT 05:26Building on the earlier point about surgical debridement, it's worth emphasizing that removing necrotic bone not only reduces bacterial load but also enhances antibiotic penetration. This synergy is crucial for eradicating chronic infections.
Kiara Gerardino
October 23, 2025 AT 06:50Honestly, if you’re still skeptical about oral therapy, you’re living in the stone age of medicine. The evidence is crystal clear, and clinging to outdated IV protocols is nothing short of medical negligence. Wake up!
John Connolly
October 23, 2025 AT 08:13Great insights everyone. I’d add that patient education on adherence is key; simple reminders and clear instructions can make the difference between success and relapse.